Whiplash Cervical Assessment 7 Indisputable Essentials
Why a Whiplash Cervical Assessment Sets the Tone for the Whole Case
For a physician, the first whiplash cervical assessment after an auto injury or chronic neck complaint is one of the most consequential measurements in the entire case. It anchors the diagnosis, shapes the treatment plan, and creates the baseline that every later visit is compared against. If that first measurement is rough, every reassessment inherits the same uncertainty.
This is especially true for whiplash and cervical injury cases. These patients often present with variable symptoms, normal imaging, and a strong subjective component. The objective data captured during the initial whiplash cervical assessment is often the clearest evidence the case will produce, and it carries weight long after the patient has finished care.
What the WAD Classification Asks Physicians to Document
The Quebec Task Force grading system for Whiplash-Associated Disorders is still the most widely used framework in chiropractic and physical medicine. It separates patients into four grades, each defined by what is found on objective examination during the whiplash cervical assessment.
WAD I describes neck pain or stiffness without measurable physical findings. WAD II adds musculoskeletal signs like reduced range of motion and point tenderness. WAD III adds neurological deficits like sensory loss, weakness, or reflex changes. WAD IV involves fracture or dislocation.
The grade a physician assigns is only as defensible as the examination behind it, which is why a structured whiplash cervical assessment workflow matters so much.
Range of Motion: The Core of the Whiplash Cervical Assessment
Cervical range of motion is the single most cited metric in whiplash documentation, and it is the heart of any credible whiplash cervical assessment. ROM loss correlates with severity, tracks recovery over time, and is one of the few cervical findings that translates cleanly to insurers, attorneys, and other providers.
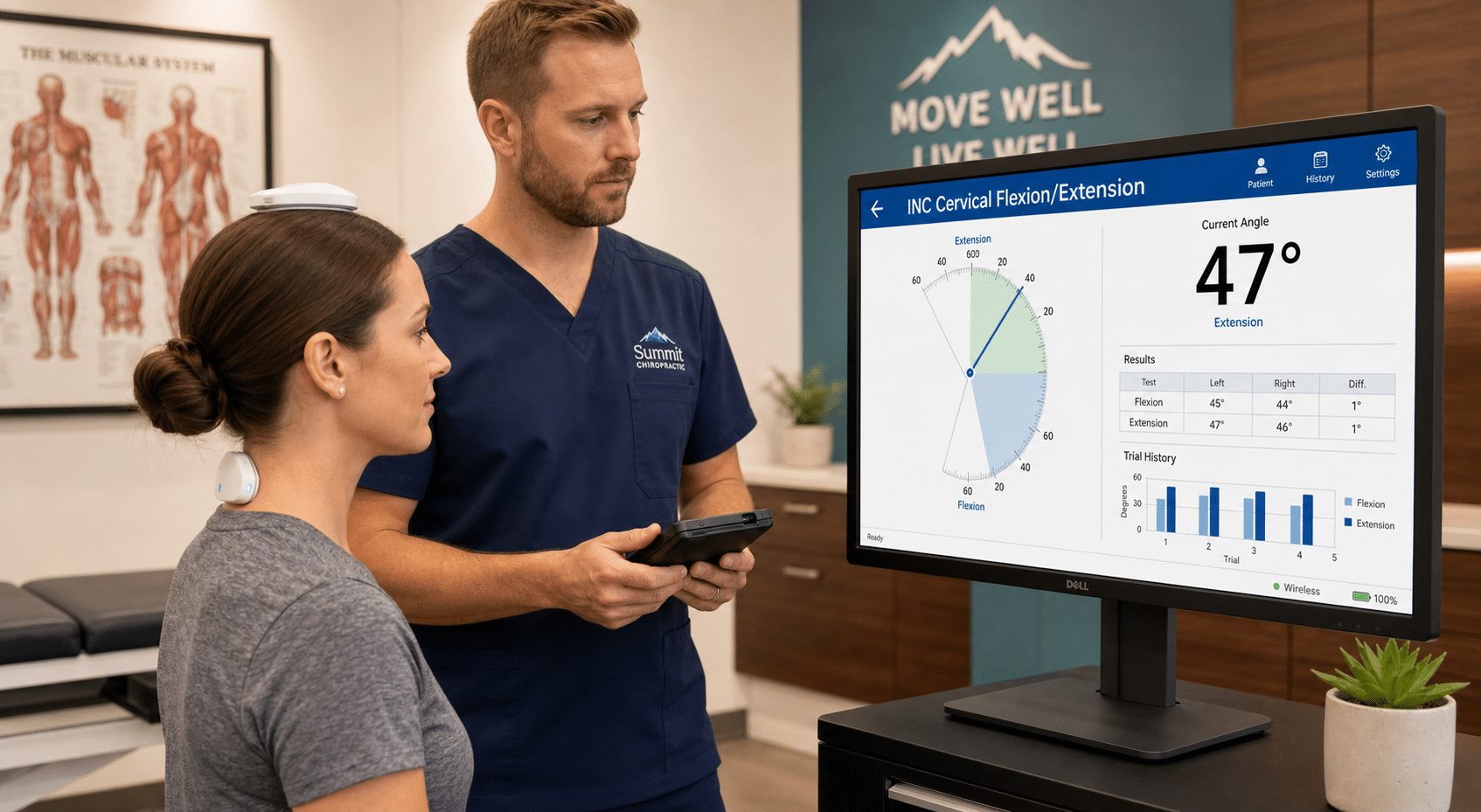
To make ROM data defensible, physicians need a repeatable measurement method. Dual inclinometer testing — performed in flexion, extension, lateral flexion, and rotation — produces consistent, validated numbers that can be compared visit to visit. Eyeball estimates and goniometer-only readings simply do not hold up under outside review.
Pain at end range, guarding, and asymmetry between sides should all be recorded alongside the raw degrees. Those qualitative notes turn a number into a clinical picture.
Neurological Screening Within the Whiplash Cervical Assessment
A complete whiplash cervical assessment also includes a focused neurological screen. Dermatomal sensory testing, myotomal strength testing, and deep tendon reflexes from C5 through T1 should be documented on every initial exam, even when the patient denies radicular symptoms.
Provocative tests such as Spurling’s, cervical distraction, and the upper limb tension test help differentiate radicular involvement from referred pain. When findings are positive, they push the case toward WAD III and change both the treatment plan and the documentation strategy.
Palpation, Posture, and Functional Findings
Beyond ROM and neuro, the whiplash cervical assessment should capture segmental palpation findings, paraspinal tone, trigger points, and postural observations such as forward head carriage or shoulder asymmetry. Functional screens — simple tasks like checking a blind spot, reaching overhead, or sustaining a neutral posture — connect impairments to real-world disability, which is exactly what insurers and attorneys want to see.
Building a Repeatable Whiplash Cervical Assessment Workflow
The fastest way to improve documentation quality is to standardize the order of operations. A repeatable whiplash cervical assessment workflow for physicians might run like this:
- Subjective intake using a validated tool such as the Neck Disability Index.
- Postural and observational screen.
- Cervical ROM with a dual inclinometer in all six planes.
- Segmental palpation and tissue findings.
- Neurological screen, including provocative testing.
- Functional and orthopedic tests as indicated.
- Documentation of WAD grade, working diagnosis, and reassessment schedule.
Running every whiplash patient through the same sequence makes findings easier to compare, easier to defend, and easier to delegate to staff for repeat measurements.
From Whiplash Cervical Assessment to Defensible Documentation
A defensible chart is not built at discharge. It is built on day one, inside the whiplash cervical assessment itself. Objective ROM values, clear neuro findings, a stated WAD grade, and a baseline outcome measure like the NDI give the case a spine that can withstand utilization review, IME challenges, or attorney scrutiny months later.
Physicians who treat the initial whiplash cervical assessment as the foundation of the case — not just an intake task — consistently produce stronger outcomes, cleaner records, and more credible reports. The exam is the case.