The Chiropractor’s Lumbar Disc Workflow: A Five-Test Battery That Beats an MRI Referral
A reliable lumbar disc workflow helps chiropractors answer three clinical questions before the patient leaves the table. Most patients who walk into a chiropractic office with low back and leg pain do not need an MRI. They need a structured physical examination that decides three things: is this a likely lumbar disc with radiculopathy, does this patient have a directional preference that predicts response to conservative care, and what objective measurements will document progress and support continued treatment? A reliable lumbar disc assessment workflow answers all three before the patient leaves the first visit — and it does it with hands, a dual inclinometer, and a structured directional-preference test, not with imaging.
Why History and Exam Still Drive the Diagnosis
Modern lumbar disc guidelines are clear that no single test is conclusive. The North American Spine Society clinical guideline on lumbar disc herniation with radiculopathy recommends manual muscle testing, sensory testing, the supine straight leg raise, the Lasegue sign, and the crossed Lasegue sign as the recommended battery for diagnosing radicular disc pain. A summary of clinical practice guidelines published in Spine Surgery and Related Research reinforces the point: the straight leg raise has reported sensitivity of 0.35 to 0.97 and specificity of 0.10 to 1.00 depending on the population and the definition of a positive test, while the crossed SLR has low sensitivity but high specificity. The clinical signal is in the combination, not in any single maneuver.
For the chiropractor, the operational takeaway is to run the same examination battery on every suspected disc case so the documentation reads consistently across patients and so each finding is interpreted alongside the others.This consistent lumbar disc workflow ensures no step is skipped.
The Five-Test Battery That Belongs on Every Suspected Disc Case
- Supine straight leg raise (SLR): passive hip flexion with the knee extended, positive when radicular pain reproduces between approximately 30 and 70 degrees. Sensitivity around 91%, specificity around 26% in classic studies — a screening test, not a confirmation
- Crossed straight leg raise: SLR on the asymptomatic leg reproduces symptoms in the painful leg. Sensitivity around 28-29%, specificity 88-90%. A positive crossed SLR is strongly suggestive of a disc lesion
- Manual muscle testing of L4, L5, and S1 myotomes: ankle dorsiflexion, great-toe extension, and ankle plantarflexion. Documented weakness raises specificity meaningfully even when sensitivity is modest
- Dermatomal sensory testing: light touch and pinprick across L4, L5, and S1 distributions. Document the side, the dermatome, and the deficit type
- Deep tendon reflexes: patellar (L4) and Achilles (S1). Asymmetric or absent reflexes add specificity to the picture
The pattern that justifies imaging or referral is rarely a single positive test — it is a positive SLR plus a positive crossed SLR plus a matching myotome weakness plus a matching dermatomal sensory loss plus an asymmetric reflex. The pattern that justifies a trial of conservative care is This decision tree is the core of the lumbar disc workflow.a positive SLR with a directional preference on examination and no progressive neurologic deficit.
Adding the Directional-Preference Examination
The single most useful addition to the orthopedic exam in disc cases is a structured directional-preference test. The McKenzie centralization phenomenon — distal leg symptoms moving proximally toward the spine in response to repeated end-range movement in one direction — is one of the strongest prognostic indicators in low back pain. A StatPearls summary of the evidence reports that centralization of low back pain occurs in approximately 58% to 91% of patients with mechanical low back pain, and 67% to 85% of those patients show a directional preference for spinal extension. The 2018 Journal of Orthopaedic and Sports Physical Therapy systematic review on the McKenzie method documents the Adding this step to the lumbar disc workflow separates mechanical responders from non-responders early.prognostic value of centralization in this population.
The clinical procedure is straightforward: with the patient marking baseline pain location and intensity, perform 10 repetitions of lumbar extension in standing, re-mark pain, then 10 repetitions of lumbar flexion in standing (or sidegliding if neither cardinal plane changes This directional-preference step completes the lumbar disc workflow examination sequence.symptoms), re-mark again. The direction that centralizes symptoms is the patient’s directional preference and the foundation of the home program.
Objective ROM as the Treatment-Response Yardstick
Even when the NASS guideline notes insufficient evidence to recommend lumbar ROM as a diagnostic test for disc herniation, ROM remains the most defensible way to document the patient’s mechanical baseline and measure response to treatment. The JOSPT clinical practice guideline for low back pain includes lumbar ROM measurement as part of the recommended examination for impairment-based classification and reassessment.
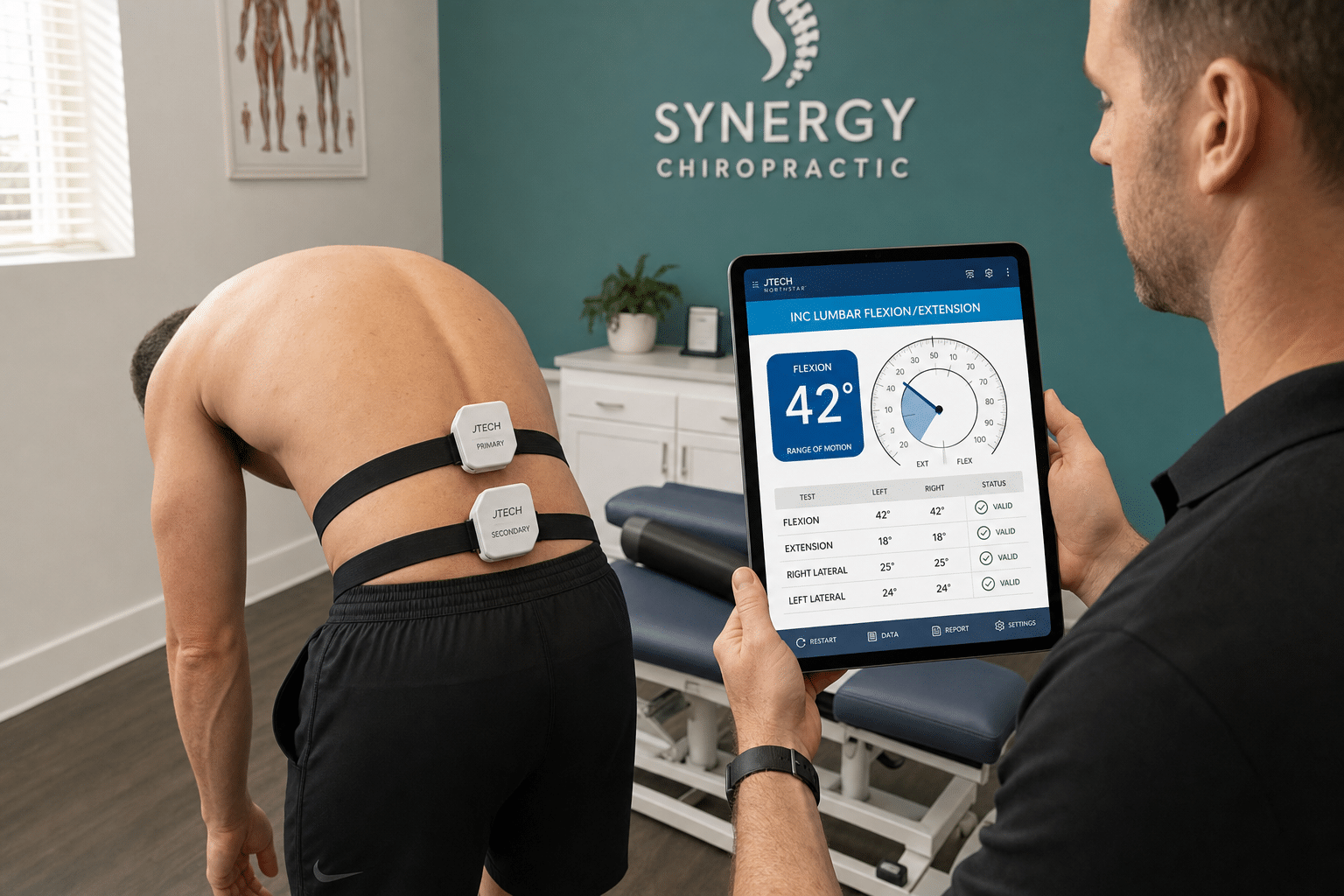
A dual inclinometer protocol — one sensor at T12-L1 and one at S2 — produces true lumbar flexion, extension, right and left lateral bending values, with the sacral contribution subtracted out. The result is a five-number snapshot at baseline and at each reassessment that is repeatable across clinicians and easy to graph over the course of care. Tools like the JTECH Northstar Echo dual inclinometer automate the math and Objective ROM data anchors the lumbar disc workflow to measurable outcomes.produce a per-visit ROM report that becomes the longitudinal record of treatment response.
When to Refer Out for Imaging
A conservative-care trial is appropriate when the examination is consistent with mechanical disc pain, the patient demonstrates a directional preference, and there is no progressive or severe neurologic deficit. Referral for MRI and surgical consultation is appropriate when any of these The lumbar disc workflow includes these referral criteria at every decision point.are present:
- Progressive motor weakness (a myotome that worsens over visits)
- Saddle anesthesia, bowel or bladder dysfunction, or other cauda equina red flags
- Severe, intractable pain unresponsive to four to six weeks of appropriate conservative care
- Recurrent radiculopathy with documented neurologic findings limiting function
- Suspected non-mechanical cause (history of cancer, unexplained weight loss, fever, IV drug use, recent trauma in osteoporotic patient)
The NASS guideline confirms that when imaging is warranted, MRI is the recommended noninvasive test, with CT or CT myelography reserved for patients in whom MRI is contraindicated or inconclusive. A well-documented chiropractic examination — positive SLR, positive crossed SLR, Knowing when imaging is warranted is a critical gate in the lumbar disc workflow.matching myotome weakness, ROM baseline — is exactly the referral note a spine surgeon or neurologist wants to receive.
How This Lumbar Disc Workflow Supports Continued Care
For the patient who is the right candidate for conservative care, the value of the workflow is in the reassessment. A two-week reassessment with the same battery — SLR, dermatomal testing, manual muscle testing, dual-inclinometer ROM, and directional-preference re-test — either documents measurable improvement (lumbar flexion 38 to 52 degrees, SLR from 35 degrees to 65 degrees, centralization of distal leg pain) Structured reassessment is what makes a lumbar disc workflow defensible or flags a non-responder for re-evaluation. Either outcome makes the medical-necessity case for the next phase of care, and either outcome reads cleanly to a third-party reviewer. For a related read on building objective findings into the documentation, see our prior post on defensible documentation.
Bottom Line
A reliable lumbar disc workflow is a five-test orthopedic battery, a structured directional-preference examination, and a dual-inclinometer ROM baseline — not an MRI. Performed in the same order on every suspected disc case, it identifies the patients who belong in a trial of conservative care, documents the patients who are improving in numbers a reviewer will accept, and flags the patients who need imaging and referral with the right clinical findings to support the consult. Build the workflow once into the intake template, train the team to run it the same way every time, and the chiropractic exam becomes both the diagnostic engine and the medical-necessity record for everything that comes next.