The Personal Injury Clinic’s Letter of Protection Workflow: How to Get Your Bill Paid at Settlement
A personal injury clinic letter of protection workflow can be the difference between getting paid in full at settlement and writing off large balances. A letter of protection is one of the most useful and most misunderstood tools in a personal injury practice. Used well, it brings uninsured or underinsured injury patients through a full treatment plan, gives the attorney a clean medical record to build a case on, and gets the provider paid at settlement. Used carelessly, it produces unpaid balances, reduced collections, and bills that opposing counsel will spend hours dismantling at deposition. The difference is workflow: how the clinic decides which patients qualify, what documentation rides with every visit, and how the file is built so the bill survives the settlement negotiation.
What a Letter of Protection Actually Is
A letter of protection (LOP) is a written agreement among three parties — the injured patient, the personal injury attorney, and the medical provider — in which the provider agrees to treat the patient now and the attorney agrees to pay the provider’s bill from the eventual settlement or verdict. A Champion Firm explainer on letters of protection in Georgia describes the structure clearly: a promise that medical bills will be paid from settlement proceeds, authorization for the attorney to pay the provider directly, and an acknowledgment that payment depends on the case’s outcome. Letters of protection are not health insurance, and they are not a guarantee. The patient remains ultimately responsible for the balance if the case does not produce a recovery, a point a Schmidt Kramer Pennsylvania attorney guide emphasizes for every patient considering the arrangement.
The LOP is one mechanism. A medical lien filed under state lien law is another, and the two are often layered. North Carolina General Statute Section 44-49, for example, gives certain providers a statutory lien against personal injury recoveries for injury-related care, provided the provider gave the attorney written notice and supplied an itemized statement or record within the statutory time period — a point summarized in a Wallace Pierce overview of NC medical lien practice. Section 44-50 caps medical provider lien claims (excluding attorney’s fees) at 50% of the damages recovered. Every state has its own variation, and the clinic’s intake process should know which mechanism is being used on each case.
Why LOP Bills Get Reduced at Settlement
The single most important thing a clinic can do for its LOP collections is to anticipate the reasons LOP bills get reduced and prevent each one. A Miller and Zois sample lien-reduction letter — written from the attorney’s side — lays out the standard arguments plaintiffs’ counsel use to negotiate a reduced payoff:
- Limited settlement funds relative to total liens, attorney fees, and case costs
- Disputed liability or causation that reduced the settlement value
- Questions about whether some treatment was related to the crash or to a pre-existing condition
- Billing or documentation issues — itemized charges, dates of service, balances, prior payments
- Excessive frequency or duration of care relative to objective findings
- A treating opinion that some portion of the care was not crash-related
Most of those vulnerabilities are documentation problems, not pricing problems. A clinic that produces a clean, objective record from the first visit forward removes most of them before the settlement letter is ever written.
The Letter of Protection Intake Workflow That Protects the Bill
A defensible letter of protection starts at intake. The clinic’s PI intake should establish, in writing, all of the following before the first treatment visit:
- A signed LOP on the clinic’s standard form, naming the patient, the attorney of record, and the clinic, with language clearly stating the patient remains ultimately responsible if the case does not produce a recovery
- The clinic’s standard fee schedule (the chargemaster) — the same fees billed to all PI cases regardless of payer source — documented in the chart
- A signed financial responsibility and disclosure form acknowledging the LOP arrangement, the clinic’s fee schedule, and the right to bill the patient if recovery fails
- A signed authorization for the clinic to release records and itemized bills to the attorney on request
- A documented history of the mechanism of injury, prior treatment for the same body region, and any pre-existing conditions
- An objective baseline examination on visit one: range of motion, strength where indicated, dermatomes/myotomes if radiculopathy is suspected, pain mapping, and any standardized outcome measures the clinic uses
A dual fee schedule — one price for cash, another higher price for PI — is a recurring reduction target. A ChiroSpring guide on dual fee schedules in chiropractic walks through the compliance considerations: clinics should be cautious about charging materially different fees to different payers for the same service, and any fee differential should be documented and defensible. The cleanest position is one chargemaster applied consistently, with cash discounts handled through a written prompt-payment policy rather than a separate price list.
What Has to Be in Every Visit Note
The visit note is what either supports or undermines the bill three years later in mediation. For each PI visit on an LOP, the chart should contain, at minimum:
- The presenting complaint, with a clear connection to the original mechanism of injury — causation language matters
- Objective findings updated at each reassessment interval — ROM in degrees, strength in pounds, dermatomal findings, palpation findings
- The treatment delivered, with CPT codes that match the documented services and time
- Patient response to treatment with measurable outcomes (centralization of radicular pain, improvement in ROM, improvement in a validated outcome measure)
- The clinical reasoning for the next-visit plan — why continued care is medically necessary
- A reassessment note at consistent intervals (every 4 to 6 weeks is a defensible cadence) that documents the trajectory in numbers
The Jim Adler attorney guide makes the practical point from the plaintiff’s side: insurers routinely argue that LOP treatment is biased, and experienced personal injury counsel counter that argument by pointing to clear, objective medical documentation. The clinic’s job is to produce that documentation by default.
Where Objective Measurement Protects the Lien
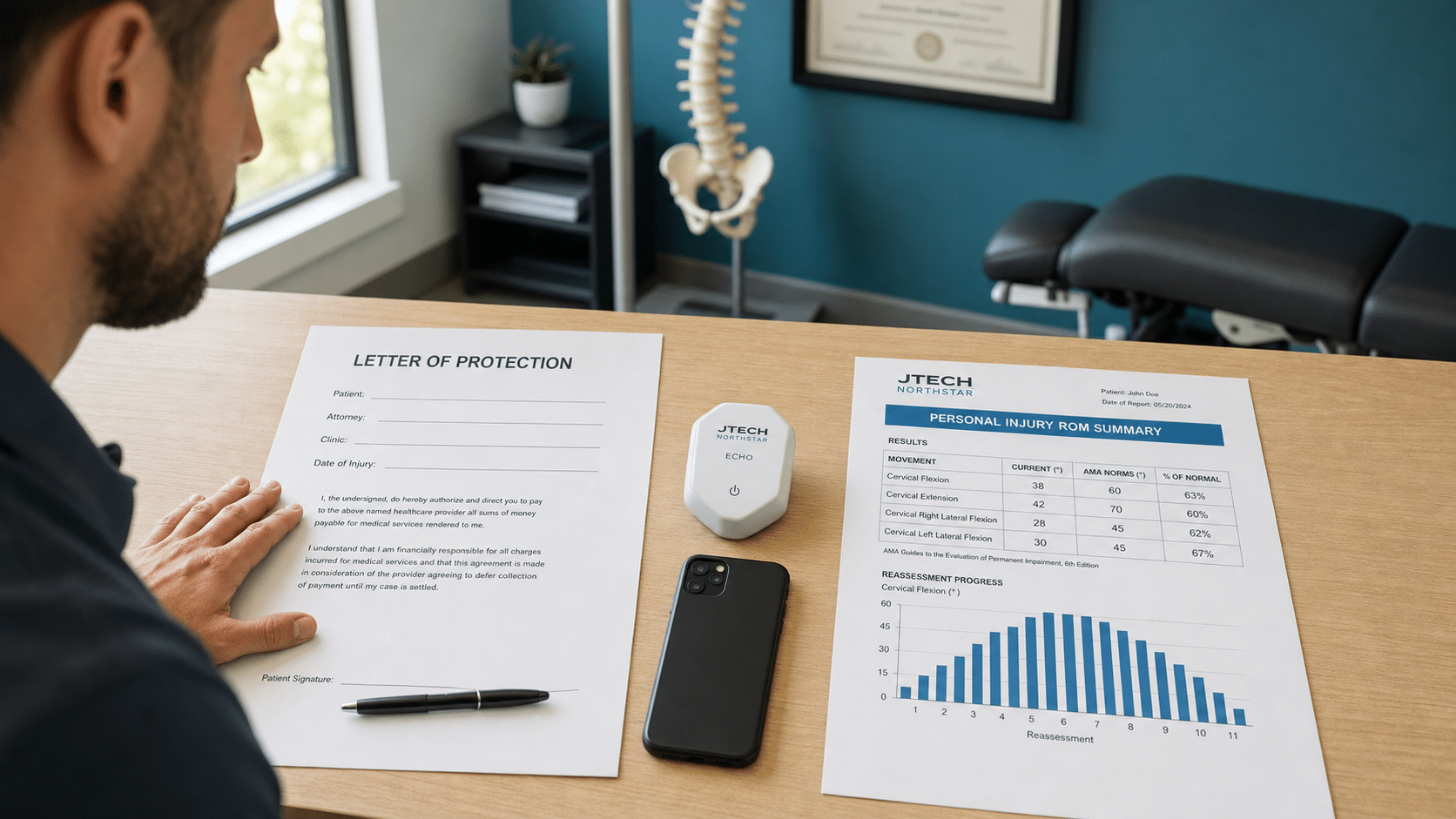
When the settlement conversation happens, the bills that get paid in full are the ones with a record showing measurable injury at intake, measurable progress through the course of care, and measurable residual deficit at discharge. ROM measured with a dual inclinometer in degrees, grip strength measured with a dynamometer in pounds, pressure pain threshold measured with an algometer in kilograms per square centimeter — these are the numbers that survive a deposition. A handwritten note saying “patient improving” does not. Platforms like the JTECH Medical Dual Inclinometers and the JTECH Medical Muscle Strength Tester generate per-visit reports with trial data, AMA-norm comparisons, and validity columns — the exact structure a reduction letter cannot easily attack.
Closing the File: Discharge and Settlement
At discharge, the clinic should produce a final report that ties the case together: the mechanism of injury, the objective findings at intake, the course of care, the response to treatment in measurable terms, the residual functional deficit if any, and a clear maximum medical improvement statement. When the attorney later requests records for settlement, the package the clinic delivers is the letter of protection, the financial agreement, the itemized bill with CPT codes and dates of service, the chargemaster reference, the intake and reassessment ROM reports, and the discharge summary. A complete package is the single biggest variable in whether the lien gets paid in full or reduced.
Bottom Line
A letter of protection is a treatment-now-pay-later agreement, not a guarantee. The bill that gets paid at settlement is the bill with a clean letter of protection, a consistent fee schedule, intake and reassessment objective findings in numbers, causation language tying treatment to the crash, and a discharge summary that reads like a clinical and legal record at the same time. Build the workflow once — intake forms, objective baseline, reassessment cadence, instrumented testing — and every LOP case in the practice runs through the same defensible playbook. A.A clean letter of protection, paired with objective documentation, is what turns a treat-now-pay-later promise into a bill that survives the settlement negotiation.