Work Conditioning vs Work Hardening: How Occupational Medicine Clinics Choose the Right Program
Work conditioning vs work hardening is one of the most consequential return-to-work decisions an occupational medicine clinic makes. When an injured worker has plateaued in routine physical therapy but still cannot meet the physical demands of the job, the occupational medicine team has two distinct tools available: work conditioning and work hardening. The names sound interchangeable, the CPT codes are shared, and in casual conversation they often blur together. Clinically and from a payer perspective, they are not the same program. Knowing which one to order, when to escalate, and how to document the objective progression is the difference between a defensible return-to-work plan and a denied claim.
Work Conditioning vs Work Hardening: Two Programs, One Goal, Different Intensity
The clearest published distinction comes from the American Physical Therapy Association clinical guidance on optimizing work participation after injury and the operational standards in the Washington Department of Labor and Industries Work Hardening Program Standards. Work conditioning is a goal-oriented, single-discipline program (typically PT or OT) that restores systemic, neuromuscular, cardiovascular, and musculoskeletal capacity. It runs roughly 2 to 4 hours per day, 2 to 5 days per week, for about 1 to 4 weeks. It does not involve vocational counseling, formal psychosocial intervention, or extensive job-task simulation.
Work hardening is the next step up. It is interdisciplinary — physical therapy, occupational therapy, and depending on the case, psychology and vocational rehabilitation. It is built around real or simulated job tasks specific to the patient’s job analysis, runs up to 4 to 8 hours per day, 3 to 5 days per week, and typically lasts 4 weeks (with documented exceptions allowed up to 6 weeks). The Washington L&I standard requires the patient to be no more than 2 years past date of injury and to demonstrate physical readiness to tolerate at least 4 hours of activity per day before admission.
Where the Programs Sit in the Recovery Continuum
Deciding work conditioning vs work hardening is easier when you map it onto the full continuum. A defensible work-injury recovery plan generally runs in this sequence:
- Acute injury management and routine physical therapy
- Functional Capacity Evaluation (FCE) to define current capacity versus essential job demands
- Work conditioning when there is a measurable strength, endurance, or ROM gap but no need for multidisciplinary care
- Work hardening when the gap is larger, the job is physically demanding or complex, psychosocial barriers are present, or the worker has been off the job long enough that fear-avoidance and deconditioning are entrenched
- Exit FCE that documents whether the worker now meets the job’s physical demand category and is ready for return to work
The entry FCE and exit FCE are what bookend either program and give the case manager, employer, and claims adjuster the objective evidence to act on. Without them, the program becomes hard to defend at audit.
Billing: CPT 97545 and 97546 Are Not Generic PT Codes
The CPT codes for work hardening and work conditioning are 97545 (initial 2 hours) and 97546 (each additional hour beyond the first 2). They are time-based and intended for the structured programs described above — not for routine therapeutic exercise. A practical guide from CareCloud on CPT 97545 lays out the documentation requirements: a documented work-related injury, defined physical and functional deficits that interfere with work tasks, an active treatment plan, and weekly reassessment using objective measurement tools. A six-week maximum is typical; care beyond that usually requires prior authorization and documented medical necessity.
An important compliance point flagged by an AAPC audit-distinction article: the multidisciplinary nature of work hardening means the constituent activities (therapeutic exercise, ADL training, etc.) cannot be teased out and billed under their own 15-minute codes — doing so is unbundling. The whole program is billed with 97545 and 97546.
What the Outcomes Literature Says
The 2017 Institute for Work and Health systematic review (Cullen and colleagues), published in the Journal of Occupational Rehabilitation, looked at workplace return-to-work interventions across musculoskeletal, pain-related, and mental-health conditions. The strongest evidence supported multi-component programs that combined health-focused interventions, service coordination, and work modification — exactly the structure of work hardening. The clinical implication for the occupational medicine clinician is that the most effective programs are not the most generic; they are the ones that target the specific job, with weekly objective metrics, and that coordinate with the employer and case manager throughout.In the work conditioning vs work hardening decision, that evidence favors the more structured, job-specific option whenever the case is complex.
Where Instrumented Testing Drives the Progression
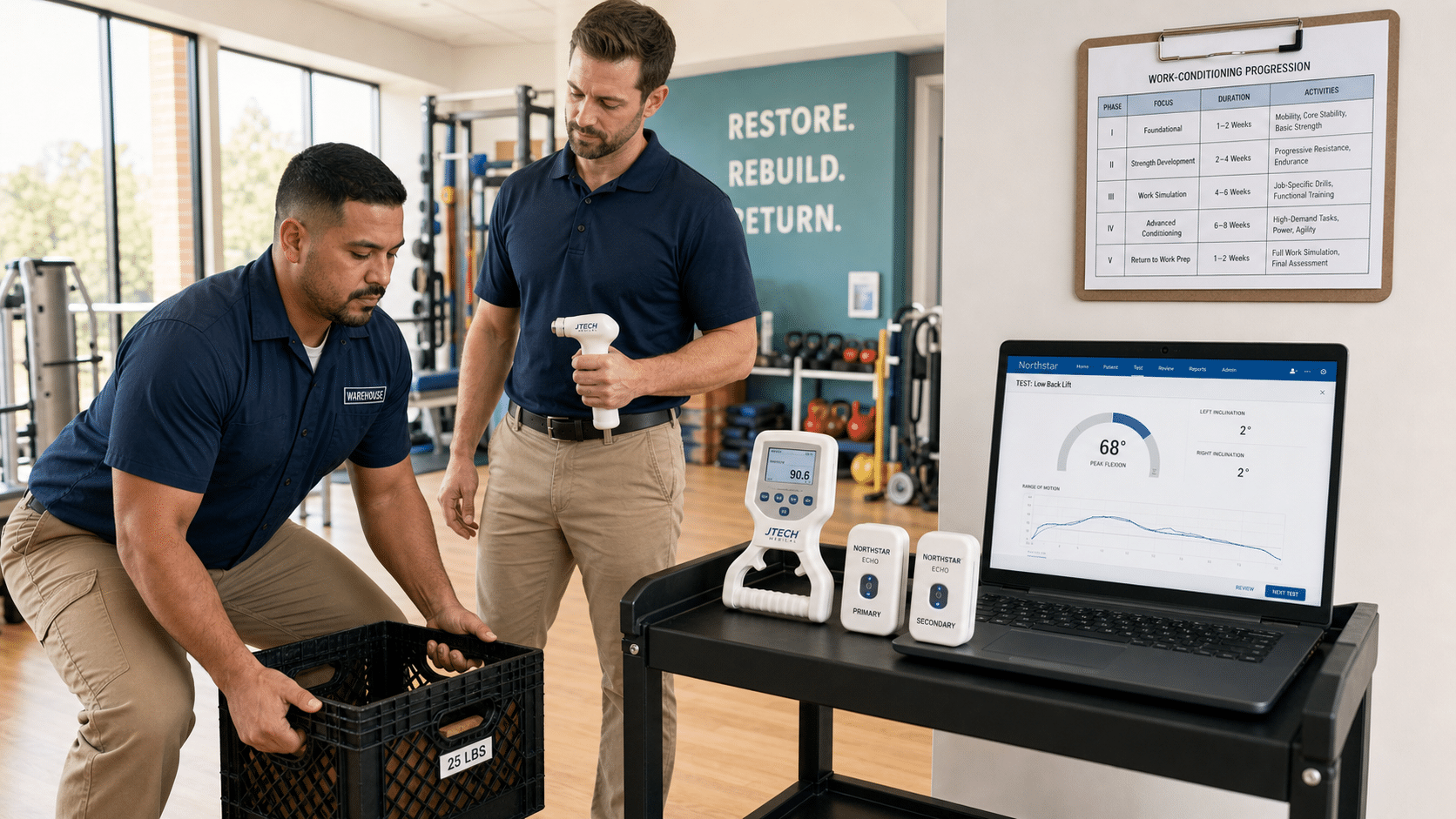
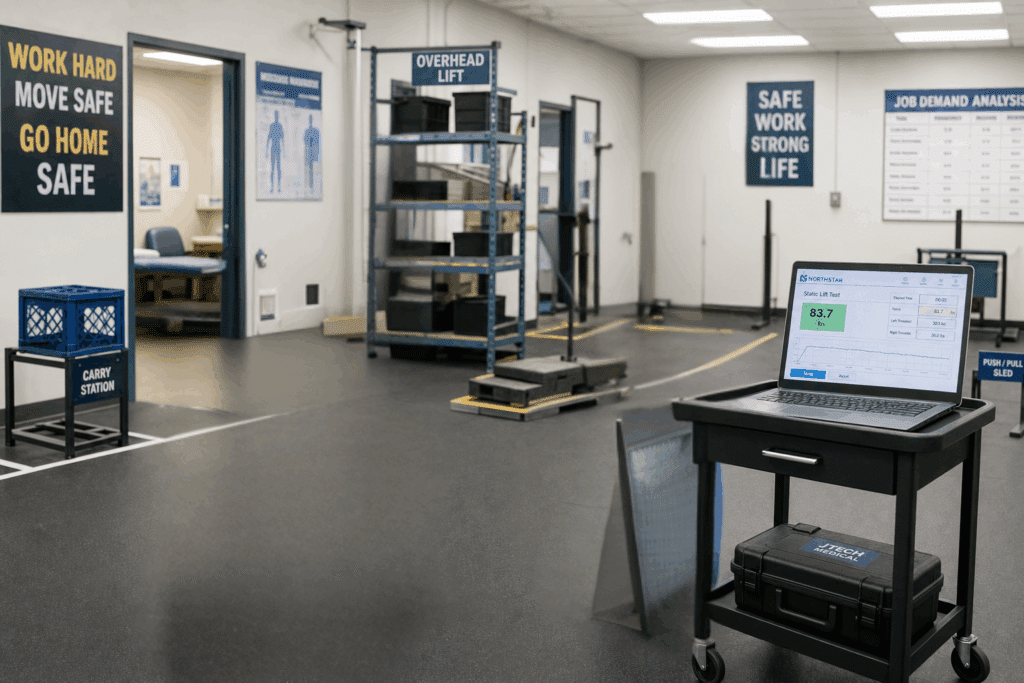
Whether you run work conditioning vs work hardening, the same rule applies. Every payer who reviews a 97545/97546 claim wants to see two things: a measurable starting deficit and weekly evidence of measurable progress. Subjective progress notes do not survive an audit. The decision to advance a worker from light load to medium load, or from 4 hours per day to 6 hours per day, has to rest on a number — not on “patient tolerated activity well.” This is where instrumented strength, ROM, and pinch/grip testing earns its place in the program. A handheld JTECH muscle tester captures isometric force in pounds with coefficient of variation across trials; a five-position JTECH grip dynamometer captures the Bell-curve grip pattern at each rung; Northstar Echo inclinometers capture cervical, thoracic, lumbar, and extremity ROM in degrees with AMA-norm comparison; the JTECH static force gauge measures lift and push-pull capacity for direct mapping to NIOSH lifting-equation job demands. All of those values flow into Northstar software, which produces the weekly trial table, force-time curves, and history bar chart that an auditor or attorney can read at a glance.
When the file shows entry FCE values, weekly Northstar reports with rising strength and ROM, and an exit FCE that matches the documented job demands, the program defends itself. The same objective record gives the attending physician the data to write a clean return-to-work release and the employer the confidence to put the worker back on the line.
Choosing Between Work Conditioning vs Work Hardening: A Practical Rubric
- Single-discipline physical deficit, motivated worker, light-to-medium job demand category — work conditioning
- Multiple physical deficits, fear-avoidance or psychosocial barriers, heavy or very-heavy job demand category, prolonged time off work — work hardening
- Patient cannot yet tolerate 4 hours per day of supervised activity — continue routine therapy, defer admission
- Patient is more than 2 years post-injury without documented exception — low expected benefit per Washington L&I criteria
- No defined return-to-work goal or job analysis on file — get those in place before admission
Bottom Line
Work conditioning vs work hardening is not a distinction without a difference, and that difference matters at the payer, in the chart, and in the courtroom. Work conditioning rebuilds the physical machine. Work hardening rebuilds the worker — physical capacity, job-task tolerance, and the confidence to walk back through the plant gate. The programs that get paid, that produce sustainable return-to-work, and that hold up under audit are the ones built on an entry FCE, weekly instrumented objective measurement, a job-demand-matched plan, and an exit FCE. When a clinic treats work conditioning vs work hardening as a deliberate, data-driven choice, the tools and the workflow are well established and the opportunity is in running them with the discipline the codes and the literature already require.